
Femoral Hernia
What is Hernia?
A hernia is a bulge that forms when the organs of the abdominal cavity push out through a weak spot in the abdominal wall. The muscles of your abdominal wall are strong and tight enough to keep the internal organs in place; but muscle weakness, previous abdominal surgery or induced pressure in the abdominal wall may result in a hernia.
What is a groin hernia?
There are two types of groin hernia,
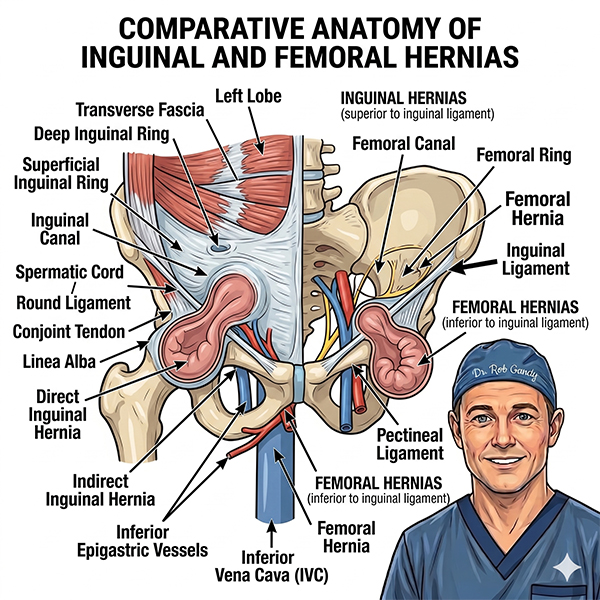
- Femoral hernia (which pass from the groin crease downwards – femoral canal)
- Inguinal hernia (which start above the groin crease and pass toward the pubic bone)
Inguinal hernias are the most common type of groin hernia and occur more frequently in men, as they follow the path of the blood vessels to the testicle (spermatic cord). If they become large they can pass into the scrotum. They can occur in men or women but are more common in men.
Femoral hernia is a less common type of hernia, about 1 in 20 groin hernias. Femoral hernia more commonly occurs in women, mostly older women, because they have wider pelvises. In a femoral hernia, the path of the hernia is adjacent to the main blood vessels to the leg (femoral canal). Femoral hernia are higher risk for strangulation than inguinal hernia.
Femoral and inguinal hernia are treated in the same fashion with hernia surgery, most commonly using laparoscopic groin hernia surgery.
What are the symptoms of groin hernia?
Most people with a groin hernia will experience pain or a lump or swelling in the groin. The lump may disappear during the day or night or only be present when coughing or straining.
In smaller groin hernias the bulge may not be visible although may still have pain. However, moderate and large groin hernias usually have a bulge that may get bigger and smaller. The pain or bulge may get worse on coughing or straining. If the bulge does not go away at any point of the day the hernia is incarcerated.
If you experience severe abdominal and groin pain or the lump is reddish and tender, there may be a chance your intestine is obstructed (stuck in the inguinal or femoral canal) or strangulated (trapped). Strangulation may block blood flow to the part of your intestine that is stuck and cause tissue death which may endanger your life. A trapped or obstructed femoral hernia may cause the following symptoms:
- Severe pain
- Nausea or vomiting
- Abdominal pain or bloating
Presence of these symptoms requires an emergency hernia repair to release the trapped tissue.
Diagnosis
Physical examination is the first line of diagnosis to test the external groin bulge. The bulge will be examined for its texture, size and protrusion. Your doctor will check for skin discolouration, inflammation or dark patches on the surface of the bulge to rule out gangrene (death of tissue). However, your doctor may find it difficult to feel the bulge if it’s small.
If the hernia cannot be detected with physical examination, your doctor may order ultrasound of the groin. Other imaging tests such as diagnostic X-rays, magnetic resonance imaging (MRI) or computer tomography (CT) scan may need be performed to check for the protruding issue.
Treatment of groin hernia
Surgical hernia repair is the mainstay of treatment groin hernias causing symptoms. Non-surgical treatments include close observation or the wearing of a truss (a type of belt that keeps the hernia from protruding).
Inguinal hernia rarely become strangulated, but are often symptomatic and will increase in size overtime. Surgical hernia repair is usually advisable, unless you have no symptoms or are unfit to undergo day surgery.
Femoral hernia usually requires surgical repair as there is a higher risk of bowel obstruction or strangulation (trapped), than an inguinal hernia. Your surgeon will push the bulged organ back to its place and close or provide support to the weakened area of the abdominal cavity.
Your surgeon may perform either an open or a laparoscopic surgery to repair groin hernia. These procedures will be performed under the effect of general anaesthesia. Local anaesthesia and medicines to help you relax may be administered for repairing a small hernia.
Laparoscopic Surgery
Laparoscopic hernia repair is now the most common chosen type of hernia repair. The exceptions are for very large hernias or hernias in people taking blood thinning medications, in which case open surgery may be safer. During laparoscopy, your surgeon will make 3 small incisions on the abdominal wall. A laparoscope (thin tube with a lighted device and a camera on its end) is inserted through one of the incisions and special surgical instruments are placed in through the other incisions. The peritoneal sac is pushed back in place and muscles of the abdominal wall are repaired by using a specially designed mesh.
Open Surgery
During the procedure, a single 4 to 10 cm long incision (this scar will often not be seen while wearing underwear or swimwear) will be made over the bulge or in your lower abdomen and the bulge will be separated from the surrounding tissues. The part of your protruded peritoneal sac will be pushed back into the abdomen. The muscles of the weak abdominal wall may either be stitched (Herniorrhaphy) or a piece of mesh may be sutured (Hernioplasty) in place to repair the hernia.
Can I Have hernia surgery without a mesh?
Yes, hernia surgery can be performed without mesh, but there is a higher risk of the hernia coming back in the future. These operations are performed in an open approach and include the Bassini, Shouldice and Desarda hernia repairs.
Complicated Hernias
Bowel resection (removal of a part of the intestine) may be required during emergency hernia surgery, if the intestine is trapped and damaged inside the hernia. Your surgeon will remove the damaged bowel and re-join the ends of the healthy bowel.